83 MOHAMMED WAHAAJ BIMONTHLY ASSIGNMENT
BELOW IS THE LINK TO THE QUESTIONS ASKED TO US:-
http://medicinedepartment.blogspot.com/2021/07/medicine-paper-for-july-2021-bimonthly.html?m=1
QUESTION 1:-
Below is the link of the student for which I am giving my peer review.
Reviews to all the questions answered:-
1) The reviews for the cases selected are well described. A detailed pinpoint review has been given to each particular case selected, which is helpful in easy analysis. Even though the peer reviews giving are short they are well described.
2)He went with good investigations and given a better explanation for every case. Even every investigation and detailed history has been correctly described in order.
3&4)A good and well-described appraisal has been provided regarding the important aspects of the case. Many useful leads and articles are mentioned so as to understand the case. The diagnostic and therapeutic intervention is one of the important aspects which is very well described.
5)My overall review of the cases he reviewed was good. we get a better understanding by studying the case. I'm sure that the patient-centered approach of collecting and learning data has been well grasped by the student.
QUESTION 2:-
https://mohammedwahaaj11.blogspot.com/2021/07/83-wahaaj_24.html
QUESTION 3:-
Case 1:-
https://krupalatha54.blogspot.com/2021/07/a-49-yr-old-female-with-generalized.html?m=1
REVIEW:-The explanation about the case was very good and gone with detailed investigations and finally got up with chronic interstitial nephritis secondary to plasma cell dyscrasias. Many serological investigations are done including LFT. 2D echo, bone marrow aspiration test is also done to identify any underlying cause for this disease.
CASE 2:-
https://srinaini25.blogspot.com/2021/07/srinaini-roll-no-33-3rd-semester-this.html
REVIEW:-This is a case of chronic kidney disease. All the identifications and investigations are headed towards the disease, as he had radiating pain towards backward. The patient went through many treatments by using different drugs to get relief.
CASE 3:-AKI Link to the case is below:-
https://laharikantoju.blogspot.com/2021/07/58-year-old-male-patient-elog-lahari.html?m=1
REVIEW:-Many investigations done which are placed very well according to date. and mentioned clear details about the case. Along with the treatment history and complaints which are described correctly for easy analysis.
CASE 4:- Patient with coma and renal failure Link to the case is below:-
https://pallavi191.blogspot.com/2021/06/gm-cases_30.html?m=1
REVIEW:-This is a bit of a complicated case as he was diagnosed with AKI secondary to UTI on CKD. They got with the diagnosis of infective endocarditis with severe AKI which is a complicated problem. Icterus and pedal edema is seen.
CASE 5:- Patient with acute on CKD Link to the case is below:-
https://kavyasamudrala.blogspot.com/2021/05/medicine-case-discussion-this-is-online.html?m=1
REVIEW:-Post TURP with non-oliguria ATN. It is a classical case where pus is seen in the urine. The patient has a history of transurethral resection of the prostate gland. Hydronephrosis is beautifully explained with MRI scans.
CASE 6:-Patient with coma and renal failure Link to the case is below:-
https://ananyapulikandala106.blogspot.com/2021/06/a-35yr-old-female-elog.html
REVIEW:-The patient was facing type 2 diabetics 3 years ago and was put on some oral hypoglycemic agents.
CASE 7:- Patient with AKI Link to the case is below:-
https://casescape.blogspot.com/2021/06/acute-kidney-injury-secondary-to.html?m=1
REVIEW:-Generalized lymphadenopathy is seen. Urosepsis is seen as there is an infection of the urinary tract. For more information regarding urosepsis refer to the below link:-
https://www.healthline.com/health/urosepsis
CASE 8:- Patient with acute on CKD Link to the case is below:-
https://rishikakolotimedlog.blogspot.com/2021/07/45-year-old-male-with-chief-complains.html?m=1
REVIEW:-Here is the patient with known Diabetics mellitus[DM] and Hypertension because of high BP.LFT and RFT are quite abnormal. HFrEF secondary to CAD is the diagnosis.
CASE 9:-Patient with AKI Link to the case is below:-
http://chavvaclassworkdecjan.blogspot.com/2021/06/pancreatitis-in-chronic-alcoholic-with.html?m=1
REVIEW:-Investigations are done well for getting a better understanding of the case. Pancreatitis occurred due to chronic alcoholism. Ultrasound is done to get a detailed view of the liver.
CASE 10:-Patient with AKI Link to the case is below:-
https://keerthireddy42.blogspot.com/2021/07/43-yr-old-male-of-nalgonda-came-to.html?m=1
REVIEW:-There are dilated veins and a distended abdomen. Alcoholic hepatitis occurred because of consuming alcohol previously. Bilateral pitting edema is seen up to the knee.
CASE 11:-Patient with acute on CKD Link to the case is below:-
https://krupalatha54.blogspot.com/2021/06/this-is-online-e-log-book-to-discuss.html?m=1
REVIEW:-The patient is with pedal edema with decreased urine output and has a history of SOB as the patient use the inhalers for 15 years. Even fever is also spiked.
QUESTION 4:-
✱ CASE 1:-https://laharikantoju.blogspot.com/2021/07/58-year-old-male-patient-elog-lahari.html?m=1
PROBLEMS:-
- lower abdominal pain: 1 week
-burning micturation:1week
- low backache after lifting weights
-dribbling/decrease of urine out put:1week
-fever :1 week
- SOB, rest:1week
INVESTIGATIONS:-
-x ray of the pelvic region to rule out any fractures or age-related bone erosion
-RFT,CBC,cue and bacterial sensitivity test to rule out UTI and viability of kidney
-USG the abdomen for ruling out any organ abnormality and fluid accumulation
TREATMENT:-
1)INJ TAZAR 2.25gm IV/ TID- antibiotic .for relieving uti
2)SYP LACTULOSE 15ml PO/TID [ To maintain stools less than or equal to 2]
✱ CASE 2:-http://srinaini25.blogspot.com/2021/07/srinaini-roll-no-33-3rd-semester-this.html
PROBLEMS:-
-Lower backache since 10days
-dribbling of urine since 10days
-Pedal edema since 3days • SOB at rest since 3days
-Increased involuntary movements of both upper limbs since 10days
INVESTIGATIONS:-
-ECG to rule out any cardiac dysfunction
-RFT to check for the functional viability of kidney
-CUE to rule out hematuria or albuminuria
-Hemogram to rule out any blood infection, anemia
-Serum electrolytes, to rule out electrolyte imbalance secondary to AKI
-USG Abdomen for ruling out any organ abnormality and fluid accumulation
-MRI brain to rule out any neural damage-causing involuntary movements
TREATMENT:-
1)Inj. PIPTAZ 2.25gm -I.V -TID antibiotics for UTI
2)Inj.Lasix 40mg I.V -BD for decreasing the fluid overload
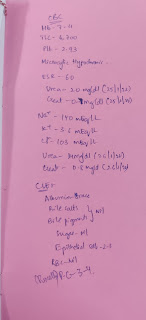
✱ CASE 3:-https://krupalatha54.blogspot.com/2021/07/a-49-yr-old-female-with-generalized.html?m=1
PROBLEMS:-
-generalized weakness.
-vomiting
-pallor ++
INVESTIGATIONS:-
-RFT to check for the functional viability of kidney
-CBC to rule out any blood infection, anemia, and cause of anemia
-since iron and vitamin b12 are normal still there's persisting anemia then bone marrow aspiration will be done to rule out and bone marrow suppression
TREATMENT:-
1) T. PAN 40mg /PO / OD decreases the gastric acid release
2) T. ZOFER 4mg / PO /SOS anti-emetics for controlling vomiting
✱ CASE 4:-https://ananyapulikandala106.blogspot.com/2021/06/a-35yr-old-female-elog.html
-Fever and Diarrhea
-Back pain( 5 days ago) with abdominal pain and chest pain
-Serum electrolytes, to rule out electrolyte imbalance secondary to AKI
-USG Abdomen for ruling out any organ abnormality and fluid accumulation
✱ CASE 6:-https://kavyasamudrala.blogspot.com/2021/05/medicine-case-discussion-this-is-online.html?m=1
INVESTIGATIONS:-
2)TAB NICARDIA XL 30mg ODNifedipine is a medicine used to treat high blood pressure (hypertension) and to prevent angina
3)TAB. GLICIAZIDE 80mg BDGliclazide is a medicine used to treat type 2 diabetes mellitus in adults
4)TAB. NODOSIS 500 mg TD treatment of metabolic acidosis
5)Cap. GEMSOLINE OD supplement for calcium, vitamin D, and zinc deficiency.
6)TAB.LASIX 40mg BD diuretics to reduce the swelling (edema) caused by too much water
1)PLENTY OF ORAL FLUIDS and ORS for fluid replacement compensating the fluid loss in diarrhea
2)INJ.METROGYL 400mg /IV/TID antibiotic and antiparasitic for controlling loose stools
3)INJ.CIPROFLOX 500mg /IV//OD antibiotics
6)INJ.OPTINEURON 1ampin 100ml NS IV/od combination of nutritional supplements that is prescribed to treat nutritional deficiency
7)TAB . SPORLAC DS PO/TID is composed of lactic acid bacilli that bear sporea probiotic used to treat diarrhea caused due toinfections, antibiotics, etc.
✱ CASE 9:-https://casescape.blogspot.com/2021/06/acute-kidney-injury-secondary-to.html?m=1
PROBLEMS:-
-Chief complaints of pedal edema
-Decreased urine output
-Fever
INVESTIGATIONS:-
-RFT to check for the functional viability of kidney
-CUE to rule out hematuria or albuminuria
-Hemogram to rule out any blood infection, anemia
-Serum electrolytes, to rule out electrolyte imbalance secondary to AKI
-ABG to check for metabolic abnormalities like acidosis or alkalosis
TREATMENT:-
1)Inj LASIX 40 mg IV/TID 1 -1 - 1 diuretics to reduce the swelling (edema) caused by too much water
2)Tab NODOSIS - XT PO/OD treatment of metabolic acidosis
3)Tab pcm-antipyretics for reducing body temp
4)Pantop 40-preventing s/e of pcm
✱ CASE 10:-http://chavvaclassworkdecjan.blogspot.com/2021/06/pancreatitis-in-chronic-alcoholic-with.html?m=1
-SOB since 2 days.
TREATMENT:-
-IV PIPTAZ 4.5 Gms. BD Piperacillin / Tazobactam antibiotics
QUESTION 5:-
In my opinion, seeing the healthcare situations and opportunities in the present time it is very right to say that "telemedicine is the need of today". With the help of telemedicine, a person having any health issue can get the most immediate and required medical advice/medication in the safety and comfort of their homes by making use of digital technologies. This elog plays a major role in this condition which gives the doctor idea about the patient's history of present illness, family history, and investigations for the diagnosis and treatment of the disease. During the span of 2months, I have experienced and seen many cases which are really helpful in a clinical way. I have learned many things during the posting session. Even I have got a chance to log for a case the experience was quite helpful for me in understanding how the system works. The General medicine department has done quite a good work in making us understand the subject. For every clinical case, they have guided us on how to study and analyze the case. I have learned how to capture patient-centered data for diagnosing the disease. I have got a chance to see the many types of investigations done in order to diagnose a disease. Along with this, I also read through several medical blogs of various systemic disorders which helped me understand several pathological changes that occurred in contrast to the physiological mechanisms that I had learned last year. Something new that I learned with this was various investigations that are to be performed with specific signs and symptoms and differentials that can be drawn from them. I learned how to blog which is definitely a prized possession for me.


Comments
Post a Comment