23 yr Old male with Bilateral Lower limb weakness.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
After going through the patient details as given by our Intern Mam through the following link..
https://vaish7.blogspot.com/2020/05/medicine.html?m=1
My analysis of the patient is as follows,
Chief Complaints:
*Bilateral Lower limb weakness.
Bilateral Lower limb weakness associated with Tingling and Numbness since 5 days.
There is also H/O Sudden fall.
As described by the patient, there is intially Paraparesis that gradually developed into Paraplegia.
Paraparesis can be due to
1. Injury
- Which is ruled out as there is no H/O trauma.
2. Vitamin B12 deficiency
- Which is ruled out as there is no Pallor suggestive of Anemina
3. PVD
- A sudden fall may be indicative of vascular cause probably due to stroke or ischemia or infarcts in the brain.
- However it can be ruled out as there is no signs of pain, claudication, skin changes in leg.
4. Neuromuscular Problem
- Since there is tingling and numbness it is more of a nerve issue.
- O/E of CNS ,
# Higher Mental Functions:
Patient is Conscious, Oriented to time place and person, Speech & Memory normal.
# Cranial Nerves: Intact
# Motor System:
Right. Left
Bulk: Normal. Normal
Tone:
UL. Normal. Normal
LL. HYPOTONIA HYPOTONIA
Power
UL. 5/5. 5/5
LL. 2/5. 0/5
Reflexes.
Superficial reflexes
Right. Left
Corneal. P P
Conjunctival P. P
Abdominal. P. P
Plantar Extensor Extensor
Deep tendon reflexes
Right Left
Biceps. 2+ 1+
Triceps. 2+ 1+
Supinator. 3+ 2+
Knee 3+ 2+
Ankle. 3+ 2+
jaw jerk. 1+. 1+
Ankle clonus PRESENT Absent
Primitive reflex - absent.
Involuntary movements - absent.
# Sensory System: Normal.
# Coordinaton: Normal
# Gait: ??
# Meningeal Signs: Absent
From the Nervous system examination mentioned above it is evident that there is
•B/L Hypotonia, Suggestive of LMN lesions
•Hyper reflexia of Knee and Ankle reflex suggestive of lesion UMN lesion above L3,L4
• Ankle clonus, suggestive of UMN lesion above S1,S2
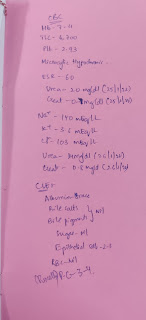
Investigations:
MRI of Spine
*Vomitings
Though patient mentioned it as a Non projectile vomiting, it is difficult to rely on patients information who might not actually know what a projectile vomiting is like.
These Vomitings may be due to intracranial space occupying lesions which causes raised intracranial pressure and vomitings.
Investigations:
MRI of Brain






*Gluteal abcess
Operated 5 months back
*scrotal abcess
Operated 10days back
These two abcess are cold abcess as there is no signs of inflammation.
Investigations:
Scraping of the abcess peripherally and send for culture to isolate the organism causing abcess.
Interpretation of Investigations:
Upon going through the investigations it is found that
There is significant enhancement which represents meningeal enhancement or exudates and following lesions in mri with multiple nodules in pulmonary apices suggest of pulmonary kochs and disseminated tuberculosis.
So the patient is now found to have Tuberculosis but didn't have any classical findings of TB.
As it is mentioned that patient has H/O Multiple Sex partners it is advised to go for HIV testing as HIV and TB co-exist. PLHIV are 21 (16-27) times at higher risk of developing TB¹.
TB Burden²

Further analysis:
•As the patient is found to have disseminated TB, it is important to ruleout TB Spine (Potts Spine)
Potts spine may cause Potts paraplegia involving both the lower limbs.
•Its is also important to ruleout Spondylodiscitis as M.tuberculosis is one of the main causative organism³.
Discussion:
•Anatomical location of the casue is most likely at the level of L3,L4.
However there must be lesion involving more than one level since the patient has features of both UMN & LMN lesions.
•Etiologically it can be due to Disseminated TB
Potts paraplegia is yet to be evaluated and ruled out.
•Pathologically the cause can be due to Clod abscess caused by MTB extending to more than one level
i.e, Above and At the level of L4,L5.
Therapeutic Options:
•Medical management
Manage TB : ATT + Rest + Taylars Brace for 18-24 months
•Surgical management
Anterolateral Decompression.
(Indicated if, No improvement with 3-6 weeks of treatment, Symptoms worsen during treatment, Bowel and Bladder involvement).
UPDATE :
•On further follow up, Upper limb reflexes were found to be exaggerated which made us to think again regarding the site of lesion,
•All the features of CNS examination now point towards UMN lesion (Hypotonia, though not a feature of UMN lesion, can be seen in acute cases of UMN lesions due to Spinal Shock).
•So now the lesion can be anywhere from Cerebral cortex to down the Corticospinal tracts.
•However here the patient has Involvement of Upper and Lower limbs without any involvement of abdominal muscles in between, we can rule out the lesion in the tracts.
If the lesion is in Tracts then there should be involvement of all the muscles below the lesion which is not happening in our patient.
• Now we can think that the lesion is in the cerebral cortex in the motor area.
• As Upper and Lower limbs are involved the lesion must be in the motor area controlling these regions, i.e., in the medial part of the Motor Homenculus.
Motor Homenculus⁴

As we can see from the above picture that the Upper and Lower limb regions are side by side a lesion in that region of the Motor Cortex can lead to involvement of Upper and Lower limbs.
• The next Question is
WHAT IS THE CAUSE OF LESION?
As the patient has Tuberculosis the MTB can cause a lesion in that area.
HOW DOES IT SPREAD TO THAT AREA?
It is through a Blood borne spread through the ACA.
Diagnosis :
TUBERCULAR ACA VASCULITIS in the medial Homenculus area of cerebral cortex
Cerebral Vasculitis secondary to Tuberculosis in previous literature
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4606267/
References:
1. India TB Report 2019,
https://tbcindia.gov.in
2. https://tbfacts.org/tb-statistics-india/
3. https://en.m.wikipedia.org/wiki/Spondylodiscitis
4. https://images.app.goo.gl/H5F68XnaVVq6Fp8s8


Comments
Post a Comment